Navigating IVF in London, Step by Step - Clinics, Costs, Treatment Options & Real Stories

Fresh vs Frozen Embryo Transfer
Fresh vs frozen embryo transfer explained - timing, protocols, and how each option affects IVF success rates, recovery, and future cycles.
THE IVF PROCESS STEP BY STEP
8/11/20252 min read
When you reach the embryo transfer stage, your clinic may suggest either a fresh or frozen transfer. Both have their place in IVF, but they work very differently - and the choice can influence your body’s recovery, the timing of your cycle, and potentially your chances of success.
What is a Fresh Embryo Transfer?
A fresh transfer happens within the same IVF cycle as your egg retrieval.
Typical timeline:
Stimulation phase: Daily hormone injections to grow multiple eggs (about 8–14 days).
Egg retrieval: Eggs collected under light sedation.
Fertilisation: Eggs are fertilised in the lab (via IVF or ICSI).
Embryo development: Embryos grow for 3–5 days (cleavage stage or blastocyst stage).
Transfer: One embryo is placed back into the uterus, usually on day 3 or day 5 after retrieval.
Pros:
Shorter time to transfer - no waiting between retrieval and transfer.
Potentially fewer cycles of medication overall.
Can feel more “natural” in terms of treatment flow.
Cons:
Hormone levels after stimulation are often high, which may affect the uterine environment.
Not suitable if you have OHSS (ovarian hyperstimulation syndrome) risk or lining issues.
Less time for genetic testing (PGT) before transfer.
What is a Frozen Embryo Transfer (FET)?
A frozen transfer happens in a later cycle - embryos are frozen (cryopreserved) after fertilisation and thawed before transfer.
Typical timeline:
Complete an IVF cycle up to embryo freezing.
Wait for the next cycle (or later) to prepare the uterus.
Embryos are thawed and transferred in a medicated or natural cycle.
Pros:
Allows your body to recover from stimulation before transfer.
More flexible timing - can fit around health or life events.
Enables preimplantation genetic testing (PGT) without delaying the transfer decision.
Some studies suggest slightly higher success rates, especially in patients at risk of OHSS.
Cons:
Slight delay before transfer.
Involves thawing, which - while generally safe - carries a tiny risk of embryo loss.
Additional cycle preparation (hormones or monitoring).
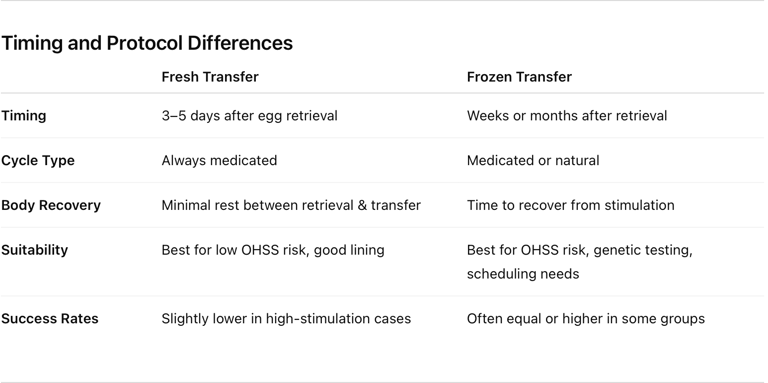
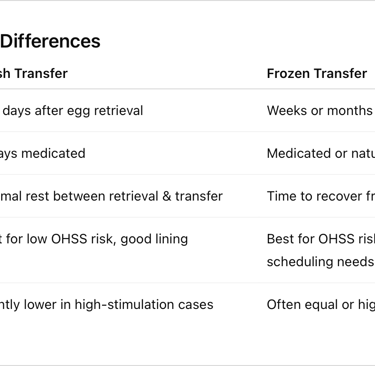
Timing and Protocol Differences
How Do Success Rates Compare?
Fresh transfers can work well, especially for younger patients with good embryo quality and no uterine concerns.
Frozen transfers are increasingly common; many clinics report similar or slightly higher pregnancy rates, particularly in patients whose bodies benefit from a “reset” between retrieval and transfer.
Success depends more on embryo quality, uterine health, and overall treatment plan than whether the embryo was fresh or frozen.
Which Option Is Right for You?
The choice is rarely purely personal - your fertility specialist will consider:
Your hormone levels after stimulation
Risk of OHSS
Uterine lining quality
Whether you’re doing PGT
Personal or scheduling factors
Some patients try both approaches in different cycles. What matters most is creating the optimal environment for implantation - whether that’s immediately after egg retrieval or in a carefully prepared future cycle.
© 2025. All rights reserved.